 Camden
Camden

 Contact us for
Contact us for Contact us for
Contact us for
Fungal Infections: Types, Symptoms, and Management
#ringworm #fungal treatment #nailfungus #dermatology #dermatologist
Fungal infections, also known as mycoses, are caused by fungi that invade and colonize various tissues in the human body. These infections can range from mild and superficial to severe and life-threatening. This comprehensive overview will explore the different types of fungal infections, their symptoms, and management strategies.
Types of Fungal Infections
More commonly, patients tend to experience superficial fungal infections. This is in part contributed by the warm and humid tropical climate locally. Certain lifestyle and hobbies involving heavy physical exertion or medical conditions e.g. diabetes, may also contribute to fungal infections.
Superficial Fungal Infections (And its close mimics)
- Tinea Pedis (Athlete’s Foot): Affects the feet, causing itching, cracking, and scaling. N.B. This can be commonly mistaken for feet eczema. Ancillary testing may be required to differentiate the two conditions.
- Tinea Corporis (Ringworm): Circular, itchy lesions on the body. N.B. Psoriasis can sometimes be a close consideration. Topical steroidal treatments, while beneficial for psoriasis treatment, may lead to a worsening of the rash.
- Tinea Capitis (Scalp Ringworm): Scalp infection causing hair loss and itching. N.B. This form of superficial fungal infection can be mistaken for both other infective causes (e.g. lice) or non inflammatory causes (e.g. Seborrhoeic dermatitis (a form of eczema affecting oilier parts of the body).
- Tinea Cruris (Jock Itch): Groin infection causing itching and redness. N.B. There are subset of inflammatory conditions e.g. psoriasis which can affect the folds. These subsets have an ‘inverse’ prefix e.g. inverse psoriasis, signifying its location over folds.
- Tinea Unguium (Onychomycosis): Fungal infection of the nails. N.B. There are different species of fungus, which one showing up as different appearances of nails. Fungal culture for proper identification and treatments are usually warranted for more targeted treatment.


Credit: American Family Physician (2013).
Subcutaneous Fungal Infections
As the name suggests, these are more deep seated fungal infections affecting the deeper parts of the skin (subcutis) and lymph hodes. A history of inoculation or cuts can sometimes preceded the development of fungal infection. Examples of such conditions are: Sporotrichosis (Infection caused by Sporothrix schenckii, affecting skin and lymph nodes.) and Chromoblastomycosis (Chronic infection affecting skin and subcutaneous tissue.)
Systemic Fungal Infections
- Candidemia: Bloodstream infection caused by Candida species
- Aspergillosis: Infection caused by Aspergillus species, affecting lungs and other organs
- Cryptococcosis: Infection caused by Cryptococcus neoformans, affecting lungs and central nervous system
- Histoplasmosis: Infection caused by Histoplasma capsulatum, affecting lungs and other organs
Management of Fungal Infections
Preventive Measures
- Good hygiene: Washing hands and affected areas regularly
- Dry skin: Keeping skin dry, especially between folds
- Avoid sharing personal items: Towels, clothing, and footwear
- Wear breathable clothing: Cotton and natural fibers
Pharmacological Management of fungal infections
There are 3 main classes of antifungals, with the use of topicals being the most common.
- Antifungal powders, creams and ointments: The choice of product texture and formulation recommended by your dermatologist takes into account lifestyle and preferences.
- Oral Treatments: Usually taken as a daily oral pill. They may have certain drug interactions with existing medications. Do inform your dermatologist should you have any other regular medications.
- Intravenous antifungals: Administered through the veins or injections, they are reserved for extremely ill patients.
Conclusion
Fungal infections are diverse and can affect various parts of the body. Understanding the types, symptoms, and management strategies is crucial for effective treatment and prevention. Consult a healthcare professional for proper diagnosis and treatment.
- Centers for Disease Control and Prevention. (2022). Fungal Diseases.
- American Family Physician. (2013). Onychomycosis: Current trends in diagnosis and management.
- Genetic predisposition: Mutations in genes involved in immune response and skin barrier function
- Immune system dysregulation: Overactive T-cells and dendritic cells trigger inflammation
- Cytokine imbalance: Elevated levels of tumor necrosis factor-alpha (TNF-α), interleukin-17 (IL-17), and interleukin-23 (IL-23)
- Environmental triggers: Allergens, irritants, and stress exacerbate symptoms
- Plaque psoriasis: Most common form, characterized by red, scaly patches
- Guttate psoriasis: Small, droplet-shaped lesions
- Inverse psoriasis: Smooth, red lesions in skin folds
- Pustular psoriasis: White pustules on red skin. It can be confluent (or joined together) to form lakes of pus
- Erythrodermic psoriasis: Widespread, severe inflammation
- Psoriatic arthritis: Joint inflammation and damage
- TNF-α Inhibitors
- IL-17 Inhibitors
- IL-23 Inhibitors
- Phosphodiesterase 4 (PDE4) Inhibitors
- Janus Kinase (JAK) Inhibitors (for Psoriatic arthritis)
- Area affected: Percentage of body surface area (BSA) affected
- Erythema (redness)
- Induration (thickness)
- Scaling
- PASI 50: 50% improvement from baseline
- PASI 75: 75% improvement from baseline
- PASI 90: 90% improvement from baseline
- Injection site reactions
- Increased risk of infections (upper respiratory tract, sinusitis)
- Headache
- Malaise or general sense of unwell
- Nestle et al. (2016). Psoriasis. New England Journal of Medicine
- Sharma et al. (2023). Annals of Phytomedicine
- Genetic predisposition: Mutations in filaggrin (FLG) and other genes affect skin barrier function
- Imbalanced immune response: Overactive Th2 cells produce cytokines like IL-4 and IL-13, driving inflammation
- Skin barrier disruption: Loss of natural moisturizing factors and impaired ceramide production
- Environmental triggers: Allergens, irritants, and stress exacerbate symptoms
- Topical corticosteroids: Reduce inflammation and itching
- Topical immunomodulators: Modulates immune response to reduce skin inflammation. Non steroidal-based
- Emollients: Hydrate and protect the skin
- Phototherapy: Ultraviolet (UV) light reduces inflammation in the skin through suppressive effects on overactive immune cells in the skin (T-lymphocytes). This can be delivered to the whole body or on specific sites via a targeted hand piece
- Leung DYM, et al. (2014). New insights into atopic dermatitis. Journal of Clinical Investigation, 124(3), 943-952
- Beck LA, et al. (2014). Dupilumab treatment for moderate to severe atopic dermatitis. New England Journal of Medicine, 371(2), 130-139
- Simpson EL, et al. (2016). Baricitinib in patients with moderate to severe atopic dermatitis. Journal of the American Academy of Dermatology, 75(3), 555-563
- Non-Inflammatory Acne – Characterized by open and closed comedones (blackheads and whiteheads respectively)
- Inflammatory Acne – Includes papules, pustules, nodules, and cysts.
- Cystic Acne- Large, painful cysts and nodules- often a more severe state of inflammatory acne
- Acne Vulgaris: Most common type, typically affecting adolescents and young adults.
- Acne Conglobata: Severe, chronic form with connected nodules and abscesses.
- Acne Rosacea: Combination of acne and rosacea symptoms
- Occupational acne (Chloracne): Exposure to hydrocarbons at work
- Medication-induced acne: Steroids, testosterone, certain birth control/ hormonal preparations
- Familial syndromes
- Systemic acne affecting other areas e.g. hidradenitis suppurativa
- Hormonal fluctuations
- Genetics
- Stress
- Poor skincare habits
- Medications (corticosteroids, testosterone)
- Diet (dairy, refined carbohydrates)
- Physical Examination: Visual inspection of skin lesions.
- Medical History: Assessing hormonal imbalances, medication use.
- Laboratory Tests: Blood tests for hormonal imbalances, bacterial infections.)
- Skin Scrapings: Microscopic examination for fungal or bacterial infections.
- Imaging Studies: Rarely used, but may help identify underlying conditions.
- Benzoyl Peroxide: Kills bacteria, reduces inflammation
- Salicylic Acid: Exfoliates, unclogs pores
- Retinoids: Derivatives of vitamin A, prevent clogged pores
- Antibiotics: Doxycycline, minocycline and erythromycin for anti inflammatory properties and bacterial infections
- Hormonal Treatments: Birth control pills, spironolactone
- Isotretinoin: Oral retinoid for severe acne
- Light Therapy: Targets bacterial growth
- Extraction: Removing blackheads and whiteheads
- Chemical Peels: Exfoliates, improves skin texture
- Microdermabrasion: Non-invasive exfoliation
- Dietary Modifications: Avoid trigger foods
- Hydration: Adequate water intake
- Stress Management and mindfulness activities: Relaxation techniques
- Skincare Routine: Gentle cleansing, moisturizing
- Journal of Clinical and Aesthetic Dermatology. (2019). Acne Treatment Options.
- Vasam et al. Acne vulgaris: A review of the pathophysiology, treatment and recent nanotechnology based advances. Biochemical and biophysics report. (2023)
#psoriasis #psoriasis treatment #biologics #dermatology #dermatologist
Psoriasis is a chronic autoimmune disease affecting millions worldwide, characterized by thick, scaly, and inflamed skin lesions. Additionally, psoriasis can have extracutaneous (beyond the skin) manifestations, affecting joints of the body. Traditional treatments may not provide adequate relief, or may only be skin directed, leading to the development of biologic therapies. This essay delves into the pathophysiology of psoriasis, its clinical manifestations, and the various biologic agents available for treatment.
Pathophysiology of Psoriasis
Psoriasis results from a complex interplay between genetic, environmental, and immune system factors. Key contributors include:
Clinical Manifestations of Psoriasis
Psoriasis presents in various forms:

A-E: Plaque (a), guttate (b), pustular (c), inverse (d), erythrodermic (e). Credits: Sharma et al. Annals of Phytomedicine (2023)
Sometimes, more than one appearance may be present at the same time.
Biologic Therapies for psoriasis
Psoriasis arise from a complex interplay of inflammatory signalling. Certain cell type e.g. T cells and signalling pathways / molecules.
Biologics target specific molecules involved in psoriasis pathogenesis. Available biologics can be classified into several categories based on the molecules they target. Broadly, there are a few categories:
Efficacy and Safety of Biologics
Biologics have demonstrated significant efficacy in clinical trials, with many showing:
– PASI 75/90: 75%/90% improvement in Psoriasis Area and Severity Index
– IGA 0/1: Investigator’s Global Assessment of clear or almost clear skin.
What is PASI Grading
PASI (Psoriasis Area and Severity Index)
A widely used measure to assess the severity of psoriasis:
Components:
PASI Response Rates:
Common side effects
N.B. A non exhaustive list of side effects include:
Conclusion
Biologic therapies have revolutionized psoriasis treatment, offering targeted and effective options. Understanding the different types of biologics and their mechanisms enables healthcare providers to tailor treatment strategies to individual patient needs. The choice of biologics will depend on the disease severity, any previous treatments and their responses, comorbidities, patient preferences (administrative route, frequency) and/or insurance coverage.
References
Eczema: Understanding the Condition and Advanced Treatment Options
#eczema #eczematreatment #eczemamanagement #IL4 #JAKinhibitors #dermatologist #itchyskin
Dr Mok Zhun Rui, Consultant Dermatologist at The Dermatology Practice- Camden, also shared in a feature article in ChannelNewsAsia about new treatments for eczema. Do check out the link below:
Eczema, also known as atopic dermatitis, is a chronic inflammatory skin condition characterized by dry, itchy, and scaly skin. It affects approximately 10-20% of children and 1-3% of adults worldwide, significantly impacting quality of life. This article delves into the pathophysiology of eczema, traditional treatment options, and emerging therapies, including IL-4/13 inhibitors and oral Janus kinase (JAK) inhibitors.

Pathophysiology of Eczema
Eczema results from a complex interplay between genetic, environmental, and immune system factors. Key contributors include:
Traditional Skin-directed Treatment Options
Systemic immunomodulatory agents
Conventional immunosuppressive agents
This class of medication have had a long track record in the management of eczema. Prior to their initiation, a series of baseline laboratory investigations will be conducted. Usually taken orally daily, these medications may have effects on the hematological, kidney or liver. Regularr surveillance with blood tests is hence important.
IL-4/13 Inhibitors
IL-4 and IL-13 cytokines play a crucial role in eczema pathogenesis. Studies have shown that eczema is caused by an inflammatory cascade of cells and signalling proteins/ cytokines. Targeting these cytokines has shown promising results in eczema management. Medications that work on IL-4 and IL-13 cytokines are usually administered subcutaneously (in the fat layer under the skin). Some common side effects include injection site reactions, headaches, nasopharyngitis and mucosal site infections e.g. conjunctivitis.
Oral Janus Kinase (JAK) Inhibitors
Janus kinases are a family of enzymes involved in the body’s inflammatory response signal transduction (JAK/STAT signalling pathway). The name is derived from the Roman figure of duality. These enzymes have similarly two domains.
JAK inhibitors modulate the immune response by blocking the activity of JAK enzymes. Clinically, this translates to less inflammation within the skin layer. Prescribed as a daily oral formulation, there are several JAK inhibitors approved for use in patients with eczema. Side effects include increased risk of infections (upper respiratory tract, herpes simplex), cardiovascular issues, headache, gastrointestinal issues
Future Directions
Going forwards, we anticipate a new era of personalised medicine. This involves tailoring treatment to individual genetic and immunological profiles. Combination treatment with the above agents can also be administered, with ongoing evaluation of clinical data.
Lastly, the skin microbiome (a complex set of microorganisms) that contributes to good skin functioning, may be a good target for the amelioration of skin quality and hence eczema.
As research continues, optimizing treatment strategies and monitoring long-term safety will remain essential.
References
#acne #teenageacne #pimples #acnetreatment
Acne is a chronic inflammatory skin condition affecting millions worldwide, causing significant physical and emotional distress. While thought of as a condition afflicting the young, acne can also occur in other age groups. It occurs when the pores on the skin become clogged with dead skin cells, oil, and bacteria, leading to various types of lesions. This article will delve into the types of acne, investigations, and treatment options available.
Different appearances of acne
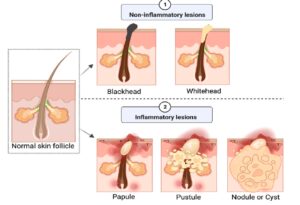
Credit: Vasam et al. Acne vulgaris: A review of the pathophysiology, treatment and recent nanotechnology based advances. Biochemical and biophysics report. (2023).
Common acneiform conditions
Be mindful that acne may also occur in adulthood, for which other causes must be elucidated. For example:
Causes and Risk Factors
Investigations
Treatment options
Topical Treatments
Do bear in mind that most acne topicals can cause skin redness, irritation and dryness. A suitable skin barrier repair cream is recommended as part of the acne skincare regimen.
Oral Treatments
Other Treatments
Lifestyle changes
Conclusion
Acne is a complex condition requiring comprehensive understanding and treatment. By recognizing the types of acne, conducting thorough investigations, and exploring various treatment options, individuals can effectively manage their symptoms and improve their quality of life. Consultation with a dermatologist is essential for personalized guidance and care.
References