 Camden
Camden

 Contact us for
Contact us for Contact us for
Contact us for
Rosacea: Understanding the Condition, Subtypes, and Treatment Options
#facialflushing #redface #centrofacial #rosaceatreatment #howtoavoidskinredness
Rosacea is a chronic inflammatory skin condition characterized by facial redness, flushing, and visible blood vessels. It affects millions worldwide, impacting quality of life and self-esteem. This comprehensive guide explores rosacea’s subtypes, symptoms, causes, and treatment options.
What is Rosacea?
Rosacea is a complex condition involving:
- 1. Abnormal blood vessel function
- 2. Inflammation
- Skin barrier disruption
Subtypes of Rosacea
The American Academy of Dermatology recognizes four primary subtypes:
- Type 1: Erythematotelangiectatic Rosacea (ETR): Persistent redness and visible blood vessels
- Type 2: Papulopustular / Inflammatory Rosacea (PPR): Redness, acne-like lesions, and pus-filled bumps
- Phymatous Rosacea: Thickened skin, nodules, and enlargement of facial features, especially the nose
- Ocular Rosacea: Eye symptoms, including redness, tearing, and burning
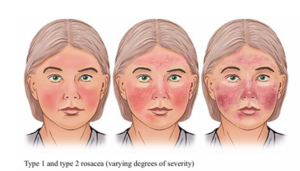
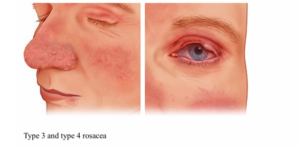
Credit: National Institutes of Health. (2023)
Symptoms
Common symptoms include:
- Facial redness and flushing
- Visible blood vessels (telangiectasias)
- Acne-like lesions
- Swelling and inflammation
- Eye irritation
- Skin sensitivity
Caution: Signs and symptoms of rosacea can be often mistaken for eczema/ dermatitis or common acne.
Causes and Triggers
Factors contributing to rosacea:
- Genetics
- Hormonal changes
- Environmental factors (sun, wind, temperature)
- Skin care products
- Certain medications
- Food and drink (spicy, hot, or caffeinated)
- Stress
Treatment Options
A comprehensive treatment plan involves:
Topicals
- Metronidazole (antibacterial and anti-inflammatory)
- Ivermectin for inflammation and reduction of demodex mites (a type of skin organism that can contribute to skin irritation and inflammation)
- Brimonidine (vascular constriction)
- Azelaic acid (anti-inflammatory and antibacterial)
Oral Medications
- Antibiotics (doxycycline, minocycline)
- Isotretinoin (severe cases)
- Beta-blockers (for flushing)
Laser and Light Therapy
- Pulsed dye laser
- Intense pulsed light (IPL)
Lifestyle Modifications
- Sun protection (SPF 50+)
- Gentle skin care
- Avoid triggers (heat, spicy food) and managing stress
Surgical Options
- Rhinophyma (severe nasal enlargement) correction
- Electrosurgery or laser surgery for telangiectasias
Conclusion
Rosacea is a complex condition requiring personalized treatment. Understanding the subtypes, symptoms, and triggers enables effective management. A combination of topical treatments, oral medications, lifestyle modifications, and laser therapy can help alleviate symptoms and improve quality of life.
- American Academy of Dermatology (AAD)
- National Rosacea Society (NRS)
- Rosacea Support Group
- Thinner skin: Pediatric skin is approximately 20-30% thinner than adult skin
- Higher water content: Increased hydration levels required, hence make pediatric skin more susceptible to dryness in normal everyday conditions
- Immature barrier function and increased sensitivity: Pediatric skin’s natural moisture barrier is weaker, hence causing it to react more intensely to irritants and allergens
- Faster cell turnover
- Thicker skin: Adult skin is more resilient due to increased collagen and elastin. In young adults, they will find their skin being sweatier or greasier, due to the maturation and increased activity of both sweat and oil glands. This can lead to acne or comedone formation as well
- Lower water content: Adult skin tends to be drier, especially with aging
- Mature barrier function: Adult skin’s natural moisture barrier is stronger, hence are more resistant to irritants
- Slower cell turnover: Adult skin regenerates more slowly
- Gentle, fragrance-free formulations: To minimize irritation and allergic reactions
- Hypoallergenic ingredients: To reduce risk of allergic reactions
- Moisturizing properties: To combat dryness and support skin hydration
- pH balanced: To maintain skin’s natural pH (5.5). Do take note that in actively inflamed or infected skin, the natural skin microbiome and pH can be disrupted. Speak to your dermatologist to see how best to manage acute flares
- Avoid harsh chemicals: No artificial dyes, sulfates, or parabens
- Glycerin: Hydrates and protects
- Ceramides: Supports skin barrier function
- Niacinamide: Soothes and calms
- Aloe vera: Soothes and hydrates
- Zinc oxide: Protects against sun damage
- Anti-aging properties: Address wrinkles, fine lines, and skin discoloration
- Gentle Exfoliating ingredients: Remove dead skin cells, promoting cell turnover
- Hydrating and moisturizing: Combat dryness, especially in mature skin
- Targeted treatments: Address specific concerns (acne, hyperpigmentation)
- Active ingredients-specific: Retinol, vitamin C, and alpha-hydroxy acids (AHAs)
- Retinol: Stimulates collagen production, reduces fine lines
- Hyaluronic acid: Hydrates and plumps
- Vitamin C: Antioxidant, brightens complexion
- Peptides: Stimulates collagen production
- Salicylic acid: Exfoliates, unclogs pores
- National Eczema Association. (2022). Skin Care for Children with Eczema.
- Journal of Clinical and Aesthetic Dermatology. (2020). Pediatric Skin Care.
- Skin Cancer Foundation. (2022). Sun Protection for Children.
- Common Warts (Verruca Vulgaris): Small, rough, and flesh-colored, often on hands and feet
- Plantar Warts (Verruca Plantaris): Painful, flat warts on the soles of the feet
- Flat Warts (Verruca Plana): Smooth, flat warts, often on face, hands, and arms
- Genital Warts (Condyloma Acuminatum): Often taking on a cauliflower-shaped appearance- these warts are found in genital areas
- Filiform Warts: Long, thin, and thread-like warts, often on face and neck
- Periungual Warts: These are warts occurring at nail margins. In view of the functional nature of our hands and feet, they may be somewhat rough, thick and/or abraded. Should the nail plate be involved, they may alter the shape of the involved nail. Periungal warts have a propensity for recurring, due to the nailplate forming a barrier which may encumber direct treatment of the wart
- Skin-to-Skin Contact: Direct contact with infected person or contaminated surfaces
- Weakened Immune System: Chemotherapy, and immunosuppressive medications
- Age: Children and teenagers are more susceptible owing to a maturing immune system/ response
- Skin Damage: Cuts, scratches, or bites provide entry points for HPV. After initial infection, warts frequently are spread by autoinoculation from scratching or shaving
- Small, Rough Growths: Typically 1-10mm in diameter
- Flesh-Colored or Pigmented: May be pink, brown, or gray
- Pain or Discomfort: Especially plantar warts
- Itching or Bleeding: Rarely, but possible
- Salicylic Acid: Over-the-counter (OTC) products
- Cryotherapy: Liquid nitrogen to freeze warts. This is a clinic administered procedure requiring regular sessions
- Cantharidin: Blistering agent derived from beetles
- Imiquimod: Prescription cream stimulating immune response
- Podophyllin: Prescription solution for genital warts
- Curettage: Scraping off warts with a curette.
- Electrocautery: Burning off warts with electrical current.
- Laser Therapy: Targeted heat to destroy warts.
- Surgical Excision: Removing warts surgically.
- Keep Skin Healthy: Moisturize and protect
- Avoid Sharing Personal Items: Towels, razors, and clothing
- Avoid Skin-to-Skin Contact: Especially over active lesions
- American Academy of Dermatology. (2023). Warts: Diagnosis and Treatment.
- American Family Physician. (2003). Molluscum Contagiosum and Warts
- Tinea Pedis (Athlete’s Foot): Affects the feet, causing itching, cracking, and scaling. N.B. This can be commonly mistaken for feet eczema. Ancillary testing may be required to differentiate the two conditions.
- Tinea Corporis (Ringworm): Circular, itchy lesions on the body. N.B. Psoriasis can sometimes be a close consideration. Topical steroidal treatments, while beneficial for psoriasis treatment, may lead to a worsening of the rash.
- Tinea Capitis (Scalp Ringworm): Scalp infection causing hair loss and itching. N.B. This form of superficial fungal infection can be mistaken for both other infective causes (e.g. lice) or non inflammatory causes (e.g. Seborrhoeic dermatitis (a form of eczema affecting oilier parts of the body).
- Tinea Cruris (Jock Itch): Groin infection causing itching and redness. N.B. There are subset of inflammatory conditions e.g. psoriasis which can affect the folds. These subsets have an ‘inverse’ prefix e.g. inverse psoriasis, signifying its location over folds.
- Tinea Unguium (Onychomycosis): Fungal infection of the nails. N.B. There are different species of fungus, which one showing up as different appearances of nails. Fungal culture for proper identification and treatments are usually warranted for more targeted treatment.
- Candidemia: Bloodstream infection caused by Candida species
- Aspergillosis: Infection caused by Aspergillus species, affecting lungs and other organs
- Cryptococcosis: Infection caused by Cryptococcus neoformans, affecting lungs and central nervous system
- Histoplasmosis: Infection caused by Histoplasma capsulatum, affecting lungs and other organs
- Good hygiene: Washing hands and affected areas regularly
- Dry skin: Keeping skin dry, especially between folds
- Avoid sharing personal items: Towels, clothing, and footwear
- Wear breathable clothing: Cotton and natural fibers
- Antifungal powders, creams and ointments: The choice of product texture and formulation recommended by your dermatologist takes into account lifestyle and preferences.
- Oral Treatments: Usually taken as a daily oral pill. They may have certain drug interactions with existing medications. Do inform your dermatologist should you have any other regular medications.
- Intravenous antifungals: Administered through the veins or injections, they are reserved for extremely ill patients.
- Centers for Disease Control and Prevention. (2022). Fungal Diseases.
- American Family Physician. (2013). Onychomycosis: Current trends in diagnosis and management.
- Genetic predisposition: Mutations in genes involved in immune response and skin barrier function
- Immune system dysregulation: Overactive T-cells and dendritic cells trigger inflammation
- Cytokine imbalance: Elevated levels of tumor necrosis factor-alpha (TNF-α), interleukin-17 (IL-17), and interleukin-23 (IL-23)
- Environmental triggers: Allergens, irritants, and stress exacerbate symptoms
- Plaque psoriasis: Most common form, characterized by red, scaly patches
- Guttate psoriasis: Small, droplet-shaped lesions
- Inverse psoriasis: Smooth, red lesions in skin folds
- Pustular psoriasis: White pustules on red skin. It can be confluent (or joined together) to form lakes of pus
- Erythrodermic psoriasis: Widespread, severe inflammation
- Psoriatic arthritis: Joint inflammation and damage
- TNF-α Inhibitors
- IL-17 Inhibitors
- IL-23 Inhibitors
- Phosphodiesterase 4 (PDE4) Inhibitors
- Janus Kinase (JAK) Inhibitors (for Psoriatic arthritis)
- Area affected: Percentage of body surface area (BSA) affected
- Erythema (redness)
- Induration (thickness)
- Scaling
- PASI 50: 50% improvement from baseline
- PASI 75: 75% improvement from baseline
- PASI 90: 90% improvement from baseline
- Injection site reactions
- Increased risk of infections (upper respiratory tract, sinusitis)
- Headache
- Malaise or general sense of unwell
- Nestle et al. (2016). Psoriasis. New England Journal of Medicine
- Sharma et al. (2023). Annals of Phytomedicine
- Genetic predisposition: Mutations in filaggrin (FLG) and other genes affect skin barrier function
- Imbalanced immune response: Overactive Th2 cells produce cytokines like IL-4 and IL-13, driving inflammation
- Skin barrier disruption: Loss of natural moisturizing factors and impaired ceramide production
- Environmental triggers: Allergens, irritants, and stress exacerbate symptoms
- Topical corticosteroids: Reduce inflammation and itching
- Topical immunomodulators: Modulates immune response to reduce skin inflammation. Non steroidal-based
- Emollients: Hydrate and protect the skin
- Phototherapy: Ultraviolet (UV) light reduces inflammation in the skin through suppressive effects on overactive immune cells in the skin (T-lymphocytes). This can be delivered to the whole body or on specific sites via a targeted hand piece
- Leung DYM, et al. (2014). New insights into atopic dermatitis. Journal of Clinical Investigation, 124(3), 943-952
- Beck LA, et al. (2014). Dupilumab treatment for moderate to severe atopic dermatitis. New England Journal of Medicine, 371(2), 130-139
- Simpson EL, et al. (2016). Baricitinib in patients with moderate to severe atopic dermatitis. Journal of the American Academy of Dermatology, 75(3), 555-563
- Non-Inflammatory Acne – Characterized by open and closed comedones (blackheads and whiteheads respectively)
- Inflammatory Acne – Includes papules, pustules, nodules, and cysts.
- Cystic Acne- Large, painful cysts and nodules- often a more severe state of inflammatory acne
- Acne Vulgaris: Most common type, typically affecting adolescents and young adults.
- Acne Conglobata: Severe, chronic form with connected nodules and abscesses.
- Acne Rosacea: Combination of acne and rosacea symptoms
- Occupational acne (Chloracne): Exposure to hydrocarbons at work
- Medication-induced acne: Steroids, testosterone, certain birth control/ hormonal preparations
- Familial syndromes
- Systemic acne affecting other areas e.g. hidradenitis suppurativa
- Hormonal fluctuations
- Genetics
- Stress
- Poor skincare habits
- Medications (corticosteroids, testosterone)
- Diet (dairy, refined carbohydrates)
- Physical Examination: Visual inspection of skin lesions.
- Medical History: Assessing hormonal imbalances, medication use.
- Laboratory Tests: Blood tests for hormonal imbalances, bacterial infections.)
- Skin Scrapings: Microscopic examination for fungal or bacterial infections.
- Imaging Studies: Rarely used, but may help identify underlying conditions.
- Benzoyl Peroxide: Kills bacteria, reduces inflammation
- Salicylic Acid: Exfoliates, unclogs pores
- Retinoids: Derivatives of vitamin A, prevent clogged pores
- Antibiotics: Doxycycline, minocycline and erythromycin for anti inflammatory properties and bacterial infections
- Hormonal Treatments: Birth control pills, spironolactone
- Isotretinoin: Oral retinoid for severe acne
- Light Therapy: Targets bacterial growth
- Extraction: Removing blackheads and whiteheads
- Chemical Peels: Exfoliates, improves skin texture
- Microdermabrasion: Non-invasive exfoliation
- Dietary Modifications: Avoid trigger foods
- Hydration: Adequate water intake
- Stress Management and mindfulness activities: Relaxation techniques
- Skincare Routine: Gentle cleansing, moisturizing
- Journal of Clinical and Aesthetic Dermatology. (2019). Acne Treatment Options.
- Vasam et al. Acne vulgaris: A review of the pathophysiology, treatment and recent nanotechnology based advances. Biochemical and biophysics report. (2023)
- Surgical excision of the visible tumour
- Processing and sectioning of the tissue
- Microscopic examination of the sections
- Mapping of the tumour margins
- Repeat excision and examination until clear margins are achieved
- High-risk tumours (aggressive subtypes, large size, or location)
- Recurrent tumours
- Tumours in cosmetically sensitive areas (face, hands, feet)
- High cure rates (up to 99% for primary BCC)
- Minimal tissue removal, preserving cosmetic appearance
- Reduced risk of recurrence
- Improved accuracy, reducing the need for additional surgeries
- Enhanced patient comfort and satisfaction (Performed in an outpatient setting with local anaesthesia. The removal of cancer and repair of the wound is all undertaken in the same day)
- Basal cell carcinoma (BCC)
- Squamous cell carcinoma (SCC)
- Other rare skin cancers (e.g., Merkel cell carcinoma)
- Emollients
- Humectants
- Occlusives
- Emollients
Akin to the cement between bricks, emollients are ingredients that fill gaps between skin cells, making skin feel smooth, soft, and supple. They help maintain and restore the skin’s barrier function. Additionally, they strengthen the skin barrier protection against environmental stressors.
Examples of emollients:
Natural Emollients_
- Oils (coconut, olive, jojoba)
- Fatty acids (ceramides, omega-3)
- Waxes (beeswax, carnuba)
Synthetic Emollients
- Dimethicone
- Cyclomethicone
- Phenyl trimethicone
- Humectants
Much like limestone bricks- a unique quality of humectants is their ability to absorb and attract water. They retain moisture from the surrounding air, drawing water into the skin. They help maintain the skin’s natural moisture balance and can leave skin feeling hydrated and plump. They further reduce the appearance of fine line and wrinkles, and are calming to dry, sensitive, or irritated skin.
Examples of humectants:
Natural Humectants
- Honey
- Glycerin
- Sorbitol
- Xylitol
Synthetic Humectants
- Hyaluronic acid
- Sodium hyaluronate
- Panthenol
- Betaine
The third piece of the puzzle (or brick wall)!
- Occlusives
Occlusives are ingredients in skin moisturizers that work like top coats on walls. They help prevent moisture loss by forming a physical barrier on the skin’s surface. In so doing, it prevents water from evaporating (Transepidermal water loss- TEWL), keeping skin hydrated for longer.
It also supports the skin’s barrier function and reduces irritation.
There are different types of occlusives. Physical occlusives form a visible, physical barrier on the skin’s surface, like a film. Examples include petrolatum. Lipid occlusives help repair and restore the skin’s natural lipid barrier. A good example includes ceramides.
Occlusives can be especially beneficial for patients looking for longer lasting hydration and protection. It is useful for dry, sensitive, or compromised skin, especially in skin conditions like eczema and psoriasis. A good occlusive is also useful for skin exposed to harsh environments.
However, some occlusives can also leave a greasy or heavy finish, and interfere with the skin’s natural excretory processes, leading to comedogenesis or acne breakouts. In addition, certain occlusives e.g. lanolin have been known to trigger a contact reaction in sensitive individuals, leading to red, flaky and inflamed skin.
Examples of occlusives:
Natural Occlusives
- Beeswax
- Lanolin
- Coconut oil
- Shea butter
Synthetic Occlusives
- Petrolatum (Vaseline)
- Dimethicone
- Cyclomethicone
- Phenyl trimethicone
Plant-Derived Occlusives
- Carnuba wax
- Candelilla wax
- Rice bran wax
- Emollients smoothen and repair the skin’s surface
- Humectants attract and retain moisture
- Occlusives retain skin moisture and reinforce the natural skin barrier
- Moisturizers combine emollients, humectants, and occlusives to provide complete hydration and protection.
- Skin type
- Skin concerns (e.g. acne, eczema)
- Formulation and texture on the skin
- Hypo allergenicity
#pediatricskin #pediatricdermatology #skincareforchildren #dermatologist #dermatology
The human skin, the body’s largest organ, undergoes significant changes throughout life. Pediatric skin, encompassing newborns to adolescents, exhibits distinct characteristics compared to adult skin. Understanding these differences is crucial for developing effective skin care strategies and products tailored to specific age groups.
Pediatric Skin (0-18 years)
There are fundamental physiologic skin differences between adults and children. Pediatric skin have the following characteristics:
(Young) Adult Skin (19+ years)

Skin Care Product Differences
There are many product formulations available. Taking heed of the different characteristics of adult and pediatric skin, there are certain useful ingredients in caring for the skin for either groups.
Pediatric Skin Care Products
We would recommend skincare products with the following properties
Key Ingredients for Pediatric Skin (Non exhaustive list)
Adult Skin Care Products
Key Ingredients for Adult Skin (Non exhaustive list)
With greater maturity, adult skin can safely tolerate different skincare ingredients. This should be tailored to the individual skin needs. Some of more commonly used ingredients include:
Conclusion
Pediatric and adult skin exhibit distinct characteristics, requiring tailored skin care approaches. Understanding these differences enables the development of effective, age-specific skin care products. By choosing products suitable for their skin type and age, individuals can optimize their skin health and address specific concerns
#wart #warttreatment #surgeryforwart #dermatologist #dermatology
Skin warts are common, benign growths caused by the human papillomavirus (HPV). They can appear anywhere on the body, affecting people of all ages. This comprehensive article explores the types, causes, symptoms, treatment options, and preventive measures for skin warts.
Types of Skin Warts
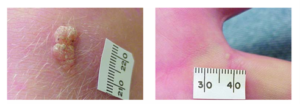
(Left: Common wart, Right: Palmar wart)
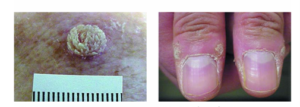
(Left: Verrucous wart, Right: Periungal wart)

(Left: Facial wart in a child, Right: Plantar wart)
Credit: American Family Physician (2003).
Causes and Risk Factors
The main etiological agent is a skin virus known as Human Papillomavirus (HPV). There are over 100 strains, with some causing skin warts.
Symptoms
Treatment Options
All treatments are hampered by wart persistence and recurrence. Sometimes, field treatment may b be offered (treating a larger area surrounding the wart).
Topical Medications
They are locally exfoliative and abrasive- helping to remove the wart burden from the top layers of skin.
Surgical Options
Vaccination
HPV vaccinations, whilst useful in the prevention management of cervical cancer, is also effective in preventing skin wart occurrence from certain HPV strains.
Home Prevention Strategies
Conclusion
Skin warts are common and usually harmless, but can be unsightly and uncomfortable. Understanding the types, causes, symptoms, and treatment options can help manage and prevent skin warts. Consult a healthcare professional for proper diagnosis and a tailored treatment programme.
#ringworm #fungal treatment #nailfungus #dermatology #dermatologist
Fungal infections, also known as mycoses, are caused by fungi that invade and colonize various tissues in the human body. These infections can range from mild and superficial to severe and life-threatening. This comprehensive overview will explore the different types of fungal infections, their symptoms, and management strategies.
Types of Fungal Infections
More commonly, patients tend to experience superficial fungal infections. This is in part contributed by the warm and humid tropical climate locally. Certain lifestyle and hobbies involving heavy physical exertion or medical conditions e.g. diabetes, may also contribute to fungal infections.
Superficial Fungal Infections (And its close mimics)


Credit: American Family Physician (2013).
Subcutaneous Fungal Infections
As the name suggests, these are more deep seated fungal infections affecting the deeper parts of the skin (subcutis) and lymph hodes. A history of inoculation or cuts can sometimes preceded the development of fungal infection. Examples of such conditions are: Sporotrichosis (Infection caused by Sporothrix schenckii, affecting skin and lymph nodes.) and Chromoblastomycosis (Chronic infection affecting skin and subcutaneous tissue.)
Systemic Fungal Infections
Management of Fungal Infections
Preventive Measures
Pharmacological Management of fungal infections
There are 3 main classes of antifungals, with the use of topicals being the most common.
Conclusion
Fungal infections are diverse and can affect various parts of the body. Understanding the types, symptoms, and management strategies is crucial for effective treatment and prevention. Consult a healthcare professional for proper diagnosis and treatment.
#psoriasis #psoriasis treatment #biologics #dermatology #dermatologist
Psoriasis is a chronic autoimmune disease affecting millions worldwide, characterized by thick, scaly, and inflamed skin lesions. Additionally, psoriasis can have extracutaneous (beyond the skin) manifestations, affecting joints of the body. Traditional treatments may not provide adequate relief, or may only be skin directed, leading to the development of biologic therapies. This essay delves into the pathophysiology of psoriasis, its clinical manifestations, and the various biologic agents available for treatment.
Pathophysiology of Psoriasis
Psoriasis results from a complex interplay between genetic, environmental, and immune system factors. Key contributors include:
Clinical Manifestations of Psoriasis
Psoriasis presents in various forms:

A-E: Plaque (a), guttate (b), pustular (c), inverse (d), erythrodermic (e). Credits: Sharma et al. Annals of Phytomedicine (2023)
Sometimes, more than one appearance may be present at the same time.
Biologic Therapies for psoriasis
Psoriasis arise from a complex interplay of inflammatory signalling. Certain cell type e.g. T cells and signalling pathways / molecules.
Biologics target specific molecules involved in psoriasis pathogenesis. Available biologics can be classified into several categories based on the molecules they target. Broadly, there are a few categories:
Efficacy and Safety of Biologics
Biologics have demonstrated significant efficacy in clinical trials, with many showing:
– PASI 75/90: 75%/90% improvement in Psoriasis Area and Severity Index
– IGA 0/1: Investigator’s Global Assessment of clear or almost clear skin.
What is PASI Grading
PASI (Psoriasis Area and Severity Index)
A widely used measure to assess the severity of psoriasis:
Components:
PASI Response Rates:
Common side effects
N.B. A non exhaustive list of side effects include:
Conclusion
Biologic therapies have revolutionized psoriasis treatment, offering targeted and effective options. Understanding the different types of biologics and their mechanisms enables healthcare providers to tailor treatment strategies to individual patient needs. The choice of biologics will depend on the disease severity, any previous treatments and their responses, comorbidities, patient preferences (administrative route, frequency) and/or insurance coverage.
References
Eczema: Understanding the Condition and Advanced Treatment Options
#eczema #eczematreatment #eczemamanagement #IL4 #JAKinhibitors #dermatologist #itchyskin
Dr Mok Zhun Rui, Consultant Dermatologist at The Dermatology Practice- Camden, also shared in a feature article in ChannelNewsAsia about new treatments for eczema. Do check out the link below:
Eczema, also known as atopic dermatitis, is a chronic inflammatory skin condition characterized by dry, itchy, and scaly skin. It affects approximately 10-20% of children and 1-3% of adults worldwide, significantly impacting quality of life. This article delves into the pathophysiology of eczema, traditional treatment options, and emerging therapies, including IL-4/13 inhibitors and oral Janus kinase (JAK) inhibitors.

Pathophysiology of Eczema
Eczema results from a complex interplay between genetic, environmental, and immune system factors. Key contributors include:
Traditional Skin-directed Treatment Options
Systemic immunomodulatory agents
Conventional immunosuppressive agents
This class of medication have had a long track record in the management of eczema. Prior to their initiation, a series of baseline laboratory investigations will be conducted. Usually taken orally daily, these medications may have effects on the hematological, kidney or liver. Regularr surveillance with blood tests is hence important.
IL-4/13 Inhibitors
IL-4 and IL-13 cytokines play a crucial role in eczema pathogenesis. Studies have shown that eczema is caused by an inflammatory cascade of cells and signalling proteins/ cytokines. Targeting these cytokines has shown promising results in eczema management. Medications that work on IL-4 and IL-13 cytokines are usually administered subcutaneously (in the fat layer under the skin). Some common side effects include injection site reactions, headaches, nasopharyngitis and mucosal site infections e.g. conjunctivitis.
Oral Janus Kinase (JAK) Inhibitors
Janus kinases are a family of enzymes involved in the body’s inflammatory response signal transduction (JAK/STAT signalling pathway). The name is derived from the Roman figure of duality. These enzymes have similarly two domains.
JAK inhibitors modulate the immune response by blocking the activity of JAK enzymes. Clinically, this translates to less inflammation within the skin layer. Prescribed as a daily oral formulation, there are several JAK inhibitors approved for use in patients with eczema. Side effects include increased risk of infections (upper respiratory tract, herpes simplex), cardiovascular issues, headache, gastrointestinal issues
Future Directions
Going forwards, we anticipate a new era of personalised medicine. This involves tailoring treatment to individual genetic and immunological profiles. Combination treatment with the above agents can also be administered, with ongoing evaluation of clinical data.
Lastly, the skin microbiome (a complex set of microorganisms) that contributes to good skin functioning, may be a good target for the amelioration of skin quality and hence eczema.
As research continues, optimizing treatment strategies and monitoring long-term safety will remain essential.
References
#acne #teenageacne #pimples #acnetreatment
Acne is a chronic inflammatory skin condition affecting millions worldwide, causing significant physical and emotional distress. While thought of as a condition afflicting the young, acne can also occur in other age groups. It occurs when the pores on the skin become clogged with dead skin cells, oil, and bacteria, leading to various types of lesions. This article will delve into the types of acne, investigations, and treatment options available.
Different appearances of acne
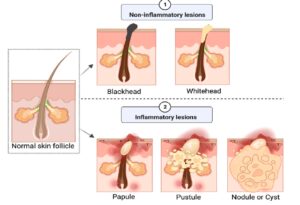
Credit: Vasam et al. Acne vulgaris: A review of the pathophysiology, treatment and recent nanotechnology based advances. Biochemical and biophysics report. (2023).
Common acneiform conditions
Be mindful that acne may also occur in adulthood, for which other causes must be elucidated. For example:
Causes and Risk Factors
Investigations
Treatment options
Topical Treatments
Do bear in mind that most acne topicals can cause skin redness, irritation and dryness. A suitable skin barrier repair cream is recommended as part of the acne skincare regimen.
Oral Treatments
Other Treatments
Lifestyle changes
Conclusion
Acne is a complex condition requiring comprehensive understanding and treatment. By recognizing the types of acne, conducting thorough investigations, and exploring various treatment options, individuals can effectively manage their symptoms and improve their quality of life. Consultation with a dermatologist is essential for personalized guidance and care.
References
#Skin cancer, #basal cell carcinoma, #Mohs Micrographic Surgery, #screening, #dermatologist
Mohs Micrographic Surgery (MMS) is a highly specialized surgical technique used to treat skin cancers, particularly basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). Developed by Dr. Frederic Mohs in the 1930s, MMS has revolutionized the treatment of skin cancer, offering unparalleled accuracy, effectiveness, and cosmetic outcomes.
History of Mohs Micrographic Surgery
Dr. Frederic Mohs, a renowned dermatologist, pioneered MMS in the 1930s. Initially, the technique involved using a zinc chloride paste to fix the tissue, allowing for serial sectioning and examination. Over the years, MMS has evolved, incorporating advancements in microscopy, histopathology, and surgical techniques. Today, MMS is widely regarded as the gold standard for skin cancer treatment.
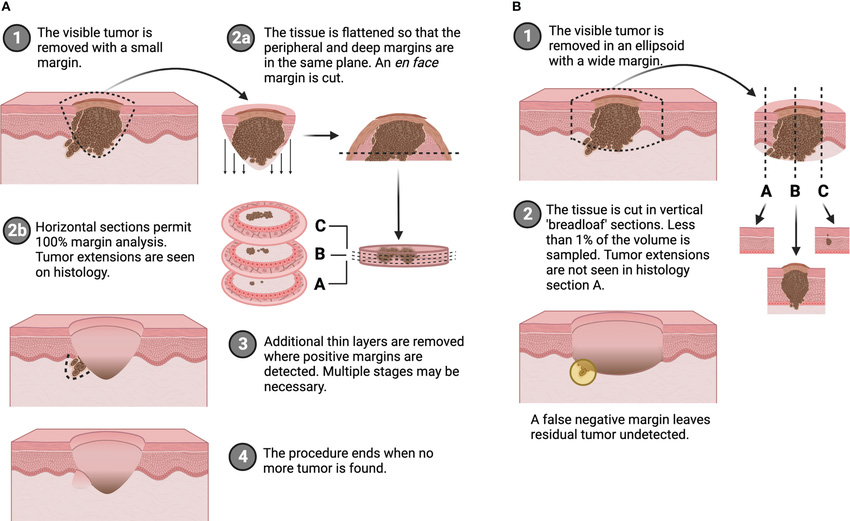
Principles of Mohs Micrographic Surgery
MMS combines surgical excision with microscopic examination, ensuring complete removal of cancerous tissue while preserving healthy tissue. This involves:
Indications for MMS include
Benefits of Mohs Micrographic Surgery
MMS offers numerous benefits, including:
Applications of Mohs Micrographic Surgery
MMS is primarily used to treat:
How is Mohs Micrographic Surgery different from conventional cancer removal surgery aka Wide Local Excision?
Mohs Micrographic Surgery (MMS) and Wide Local Excision (WLE) are two surgical techniques used to treat skin cancer. Here are the main differences:
| Mohs Micrographic Surgery | Wide Local Excision | |
| Tissue removal | Removes cancerous tissue in stages, examining each layer under a microscope until clear margins are achieved | Removes a larger area of tissue around the tumour in one go, with a predetermined margin |
| Surgical margin control | Provides 100% margin control, examining the entire tumour margin | Sampling regular sections of tissue to ensure clear margins |
| Tissue Preservation | Narrow margin control allows for healthy tissue preservation, reducing cosmetic impact. | May remove more healthy tissue, potentially leading to larger scars |
| Cure rates | Higher cure rates (up to 99% for primary BCC) | Lower cure rates (around 90% for primary BCC) |
| Surgical Time | Typically longer procedures – performed in stages over several hours | Generally shorter procedures (30 minutes to 1 hour) |
| Specialised training | Requires specialized training and expertise for surgeon and assisting surgical team | Can be performed by a wider range of surgeons |
| Tumour specific factors | Cosmetically sensitive areas (Face, hands, feet) AND/OR high-risk subtype | Low-risk tumours, smaller lesions, or tumours in less critical areas. |
Conclusion
Mohs Micrographic Surgery has transformed the treatment of skin cancer, offering unparalleled accuracy, effectiveness, and cosmetic outcomes. Its evolution over the years has solidified its position as the gold standard for skin cancer treatment in critical skin sites. As skin cancer incidence continues to rise, the importance of MMS in modern dermatological practice cannot be overstated. Patients and healthcare professionals alike can rely on MMS to provide the best possible outcomes for skin cancer treatment.
#sensitiveskin, #skincare, #dermatology, #dermatology, #eczema #acne
Moisturizers are an essential component of any skincare routine. Rather than an entity with a singular ingredient, moisturizers combine distinct skincare components to provide that soothing and hydration feel to your skin.
3 important components combine to form a good moisturizer.
These components can also have overlapping properties, providing synergistic improvements in the skin.
Imagine a brick wall with skin cells being individual bricks ….
In summary
Final tips
When choosing a moisturizer, consider 4 main aspects of your skin
By understanding the intricacies of these components, you can make informed decisions to support your skin’s unique needs and achieve healthy, radiant skin!